
The Seventh Station of Short-term Healthcare Related Missions Outreach

Critiques have been mounting with regard to the effectiveness of short-term healthcare-related missions (STHRM) trips (short-term meaning between one day and two years, though a standard has not been established). It is possible that the majority cause more harm than produce a long term good. Some believe they are mostly designed to give the participants a sense that they have made a positive contribution to the well-being of those they served. But this author has found no article written nor research conducted as to the effectiveness of STHRMs to address the needs of the whole person. Is it possible to carry out whole person care in the context of a STHRM trip? In personal communications with a ministry working in a South East Asian context I believe the answer to this question could be YES, IF … . I will define how this can be done using the term “The Seventh station” which is derived from the work of the afore mentioned ministry. I will not be revealing any details of the location and name of this ministry because of security issues. I would add that the following approach has catalyzed significant and growing movements to Jesus in that context.
A brief description of the principles employed by this ministry is in order. The work was based on the collaborative effort of five teams averaging ten people in each.
The first team was from outside of the host country and was half medical staff and funded the clinic.
The second team was made up of bilingual speakers living in the host country, both expats and those born in country. This team translated and created the connections which established and coordinated activities with the three fully Indonesian teams. This team also staffed the pharmacy and did physical therapy. Added to this team were an equal number of local healthcare professionals to match the number of expat healthcare staff, and this provided political strength in the way things looked.
The third and fourth teams were from two regions of the host country, comprised of local workers who are active in both community development as well as multiplying small community of faith groups. These were the teams with long term ministry in the areas, who had invited the other three teams to support them in the short term. The three teams agreed before coming that the success of their short-term ministries would depend on how well they maximized the ministries of the two long term teams. They agreed to adjust their typical processes in order to follow the lead of these long term local teams.
The leaders of the two long term teams had negotiated partnerships with local hosts for each day of the clinic. These local hosts were Muslims who were heads of different government entities and were responsible for getting permissions. The local long-term leaders invited selected participants to the clinic by rationing out tickets. They chose important government officials to get their endorsement, the medically needy locals who were leaders of small believer groups, their contacts with whom they planned to follow-up and form new groups (improving the likelihood of conserving the fruit), and the long-term team members.
The members of the fifth team were trained as counselors and manned the “consultation room,” the last of seven stages of the clinic. Some members of the long-term spiritual multiplication teams were trained in counseling, and other experienced counselors were added. Cross mentoring occurred in the consultation room during the short-term clinic. See diagram below for more detail on the other six stations.
Other pertinent principles:
Choose location carefully.
One reason for the effectiveness of this approach is due to the choice of the locations, that is, only locations were chosen where there were local partners who would select high value prospects to be those served and then do the follow-up. A second feature of location choice is there should be sufficient social capital with the local officials who hosted the team. They had sufficient social power which would form an umbrella of support and protection and which would increase their own social capital. This made the clinic mutually beneficial. A third feature is that the sites were considered relatively neutral and could tolerate having expats in comparison with other locations in the region.
Good administration of the healthcare outreach is key.
Another reason for success is the way the healthcare clinic was run. By the third year, everything had been evaluated and adjustments made so that the processes ran smoothly. One critical mark of success was that everyone who came was served. A mark of quality was that the attitudes of our people were felt to be centered on serving the local people and this was noticed by those being served, there was kindness felt and this helped develop trust. A third crucial element in good administration is that the flow of the patient movement through seven stages is such that it assures that individuals make it all the way through to the end stations. Also, it is designed so that there is constant interaction between the staff and the patients which facilitates personal connections being developed throughout.
Appropriate attitude of the foreign healthcare professionals is key.
Foreigners serving on these teams must come with an attitude of serving and getting behind the local leadership teams rather than running their own program. The philosophy is that short-term teams serve long-term goals determined by the long- term local workers. This has been a make or break feature of these clinics. This is a paradigm shift from the mindset of most short-term teams, who tend to underline what they can do or have done during the clinic, without realizing the impact on the local teams who face the big risk and do the lion share of the work before and after in the follow-up. Being able to bring in qualified short term teams gives the local leadership team a real boost in their service, if the short-term team aligns with their leadership in the field. A key feature to get this is a very reliable multiyear partner living in the US, who comes each year and orients the rest of the expats to this mindset which is invaluable.
Another principle that bears fruit is disciplined and earnest follow-up.
Those who participated as part of the local healthcare teams would revisit the patients multiple times and had a lot of social space for deepening of relationships. During this period, effort is made to move from individuals given whole person care during the clinic, to their social groupings they gather to discuss the Bible’s view of how Jesus cared for the whole person. However, follow-up can be made more difficult by mistakes made during the clinic.
A local study of the socio-political capital building and use is helpful.
It makes sense to the local workers to bring in foreign healthcare workers, even though they have a negative view of them, since they respect their medical capacity.
The “Seventh Station” As a Means Toward Whole Person Care (WPC)
What is whole person care? One definition is as follows: “We define “whole-person care” as the coordination of health, behavioral health and social services in a patient centered manner with the goals of improved health outcomes, more efficient and effective use of resources.1
PRIME, Partnerships in International Medical Education, doesn’t claim to define WPC as such, stating only that “At its most simplistic it is the balance between the body, mind and spirit that make up the individual.”2
Duke University prefers to express whole person care as Integrative Medicine: “Integrative medicine includes the full spectrum of physical, emotional, mental, social, spiritual, and environmental factors that influence your health. This comprehensive, customized, whole-person approach to health care is beneficial, whether you want to maintain optimal health or you are coping with a chronic condition. In both cases, our services improve how your physical body interacts with your psychological and emotional well-being.”3
For our purposes, we will use the following: whole person care involves addressing the needs of all aspects of our existence as humans. This includesthe elements of spirit, soul and body in the context in which we live.
It seems likely that this would be extremely difficult to do considering the way in which the majority of STHRMs are conducted. But we believe it is possible and that the model described above is a step in the right direction. The flow of the clinic:
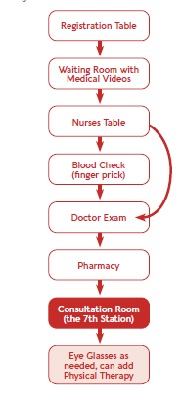
The Seventh Station Elements
- This is where the final elements of whole person care can take place.
- The staff in this station are locals only (to reduce accusations of proselytizing by expats).
- The staff are trained and experienced in both counselling and in multiplication of small communities of faith.
- The staff start with the question, “I see on your medical chart that you are suffering from… high blood pressure, for example). Are there any factors in your life that are causing you emotional, social or spiritual pressure that might be affecting your blood pressure?”
- The issues addressed in this station are:
- questions to transition from physical condition to whole person issues,
- questions or statements to transition from whole person condition to prayer for solutions that God gives,
- questions to transition to follow-up, in their natural social groupings.
- Follow-up and follow through are crucial elements after this station. This is done by the people who brought or hosted them, who had already been trained to do so.
- As a result of the seventh station, we can address the needs of the whole person; soul/spirit/body and their social conditions.




comments